FORMAL HEARING TESTS
All the formal tests make use of instruments which can vary from simple to most sophisticated ones. The tests are characterised by presentation of a sound stimulus such as puretones, speech, warble tones, noise and elicitation of a time locked response from the adult or child to be tested. The tests are performed by an audiologist (Tester) on subjects with or without hearing loss .The tests give a result, which is again interpreted by the tester. The ultimate goal of each test is to establish the auditory/hearing threshold, which is the minimum stimulus level that elicits a response consistently. These tests can be used for both screening and diagnostic purposes. These tests can be used for school screening programs also.
Prerequisites for Formal Test:
- Case History/Parental Interview
- Otoscopic examination of ears- to ensure clean ears, no infection/discharge, no ear anomaly
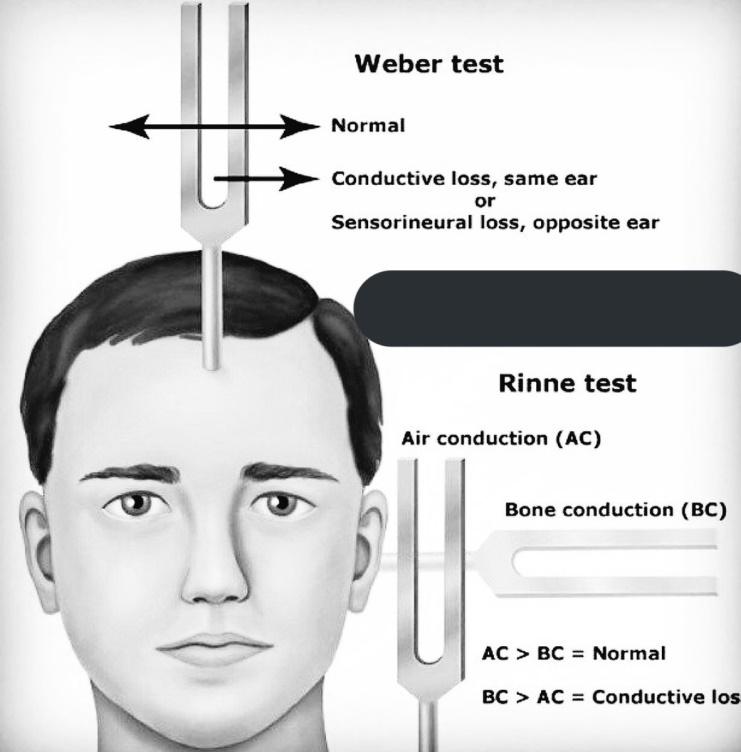
- Tuning Fork Test - can be performed by using tuning forks in older and cooperative children to get an idea about probable site of pathology (middle ear or inner ear)
- Selecting and deciding on the tests to be administered- Usually it is important to use a test battery approach in case of infants and children. This is because; it is often difficult to obtain reliable and complete results from any one particular test. So more than one test should be administered depending on the child's age, hearing status, cognitive status and economic status.
e.g For a child BOA, IMMITTANCE AUDIOMETRY AND ABR/ASSR can be administered for correct threshold estimation.
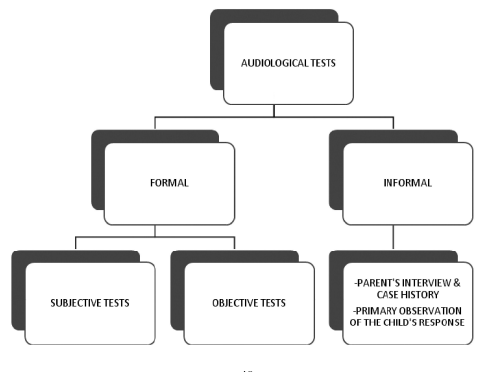
Subjective Tests
As the name suggests these tests need participation of the subject. The participation can be active or passive. In these tests the response is recorded after the presentation of a stimulus. The response can be a predefined active one,e.g. raising hand in response to a sound stimulus,or it can be a change in behavior of the child, e.g. searching for the sound stimulus or startle response which can be noted by the tester.
Behavioural Observation Audiometry
For children under six months we can use Behavioural Observation Audiometry (BOA) to test their hearing. In this type of test, the child’s behavioural responses to sound are assessed. Behavioural responses may include startling to loud noises, stirring from sleep in response to a sound, stopping sucking when a sound is heard or trying to look to the sound. An assortment of noisemakers, such as crunching cellophane, tiny bells, chimes and bicycle hooters, are used and most can be classified as low, mid or high-frequency sounds. The loudness of the sound is measured with a sound level meter. Although hearing levels cannot be determined exactly, an experienced audiologist can obtain a great deal of information from this procedure about the severity of a hearing loss and the child’s ability to detect different sound frequencies. This procedure tests both ears at once as the child does not wear headphones. Once the child has good head control and can localise sound (turn to where a sound is coming from), a more advanced procedure can be used.
Visually Reinforced Orientation Audiometry
Visually Reinforced Orientation Audiometry (VROA) involves the child turning towards a loudspeaker whenever a sound is presented. When the child looks to the speaker, a puppet or some other visual reward is given. Children soon learn that when they hear the sound, the puppet is there if they look around. From this procedure, accurate hearing thresholds can be obtained. As VROA is usually performed without headphones, individual ear information is not available. However, individual ear results can be obtained if the child will wear head phones. Most children enjoy this game and soon learn its rules.
VROA is used from when the child is about six months until the time their concentration span is long enough to move on to play audiometry (usually two-and-a-half to three-and-a-half years).

Play Audiometry
Play audiometry works the same way as pure tone audiometry described earlier except, on hearing a tone, the child puts a marble in a marble race, presses a computer keyboard to make something happen, or puts a piece in a puzzle. Making a “game” of the tests keeps the child’s interest and enables a larger number of thresholds to be obtained. This style of testing is sometimes called stimulus-response testing where the pure tone is the stimulus and the child’s action (putting a marble in a race) is the response. As the child wears headphones for this test, individual information from both ears is obtained.
Pure Tone Audiometry
Pure tone audiometry is a routine audiometric test used to measure auditory threshold of an individual in a sound proof test room. The instrument used in this measurement is known as the audiometer. This is a subjective investigation, the accuracy of which is dependent on the response of the patient. It can be used for children 5 years and above.Pure tone audiometry provides information about the type of hearing loss and also helps in quantifying frequency specific threshold. This test is generally performed with headphones for air conduction testing (AC) and bone conduction vibrator for bone conduction testing (BC). Simple pure tones varying in frequency from 250 Hz to 8000 Hz;and varying in intensity from 0 dBHL to 120 dbHL are used for testing. However the frequency and intensity range depends on the test. For example,in case of BC testing,the measurement is done from 250 Hz to 4000 Hz. The intensity range is also maximum up to 85 dBHL. With the help of a particular pattern/sequence of presenting the puretones, the ear specific threshold across all the test frequencies is established and plotted on an audiogram.
SPEECH AUDIOMETERY
As the name suggests, the stimulus or signal used for this test is speech. Speech audiometry is an additional test, which is done to confirm the results of pure tone audiometry. Moreover it gives an idea about difficulty in real life situation where the most important stimulus to be heard is human speech. A pure tone audiometer is used for this testing, when the speech is presented live,the tester speaks in the microphone attached to the audiometer which can be heard by the child wearing headphones,or through loudspeakers in the test room. The speech signal can also be recorded and presented using a CD player which can be connected with the audiometer. The speech stimulus can be monosyllables or PB words like /pa/, /cha/, /sha/, word pairs called spondee like /ma-baap//aaj-kaal/the child has to repeat the stimulus upon hearing,or they can write it down. Younger children can also point out picture cards corresponding to the stimulus words or sentences.

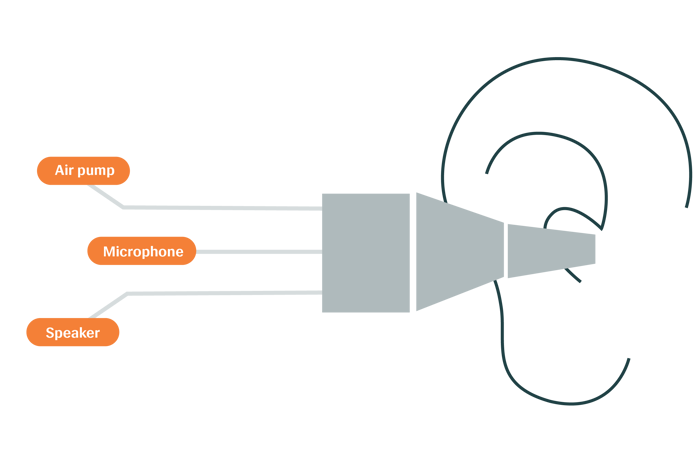
Immitance Audiometry
Also known as impedance audiometry, it is an automatic and objective means of assessing the integrity and function of the peripheral hearing mechanism. The impedance audiometer helps to determine tympanic membrane mobility,middle ear pressure, Eustachian tube functioning, continuity and mobility of middle ear ossicles,acoustic reflex threshold(8th and 7th cranial nerve function) and non-organic hearing loss. During a tympanometry test, a small probe consisting of an air pump, a microphone, and a speaker is placed in the ear canal. The probe size will vary depending on the patient as it must seal the ear canal completely during testing. Air pressure in conjunction with a pure tone will be introduced by this probe. Responses to this tone are measured and several values are obtained including ear canal volume, compliance or static admittance, and the tympanometric peak pressure point. These values are traced onto a graph and interpreted by a clinician to determine how well the middle ear is functioning.
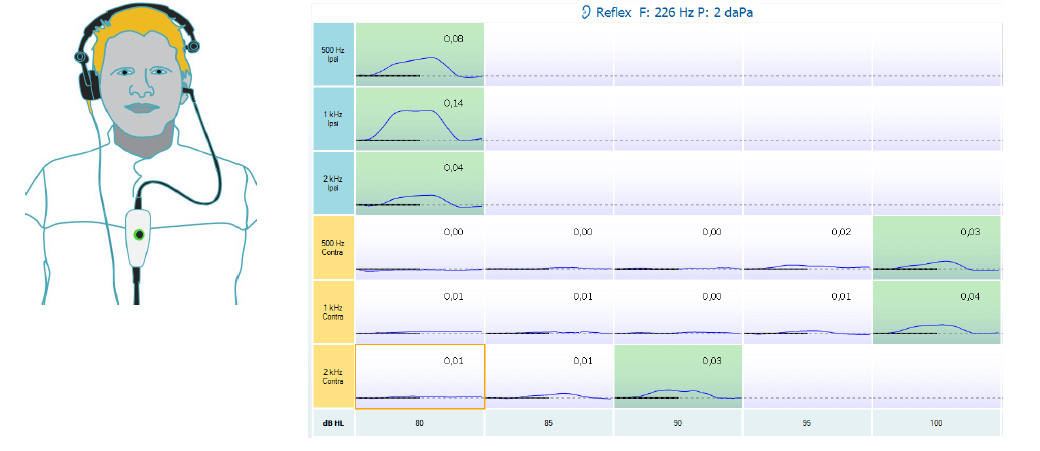
Acoustic Reflex Thresholds (ART)
The acoustic reflex is an involuntary contraction of the stapedial muscle in response to loud sounds. When the stapedial muscle contracts, it stiffens the ossicles and tympanic membrane decreasing admittance, or the absorption of sound. This stiffening can be measured in the same way as during tympanometry. During ART testing, loud sounds (70 – 115 dB), typically presented at 500, 1000, 2000, and at times 4000 Hz are introduced into the ear alongside a constant probe tone. These loud sounds induce the acoustic reflex while the probe tone detects the contraction.
Brainstem Evoked Response Audiometry
Also known as Auditory Brainstem Evoked response measurements provide information about functioning of peripheral hearing system and hearing upto brainstem level. This objective test helps in hearing assessment and also helps to locate the site of a particular lesion along the auditory pathway. A stimulus called click or tone burst is given through headphones/insert earphones and the response is recorded from the electrodes placed on various positions on the scalp of the child. There is continuous ongoing activity in the brain, an introduction of sound in the auditory path, causes a change in this ongoing activity and this can be recorded in a form of waveform. This testing is best done when the child is calm or asleep. This test can also be used for hearing screening programs in NICU.The test is carried out using a BERA instrument. The test also aims to determine the threshold of hearing, however the results obtained are interpreted and deduced in order to get the actual threshold of hearing. The waveform obtained is denominated with certain peaks(I-VI).The lowest intensity upto which peak V can be identified is defined as the threshold obtained from BERA and is usually 15 dB above PTA threshold.

Otoacoustic Emissions
Otoacoustic emissions are low level, inaudible sounds produced in the inner ear. Further these can be elicited and recorded from ear canal on introduction of external sound. This is quick procedures. The instrument consists of a probe assembly, to deliver tone and record responses at the same time from the ear canal. The presence of response indicates intactness of some part of inner ear; however the response can get affected by middle ear pathologies, presence of wax in ear canal etc. Used both as screening and diagnostic purposes. Children who fail in this test are referred for further testing. This test is also used as a part of test battery. Diagnostic tests can be Transient Evoked OAE (TEOAE) or Distortion Product OAE (DPOAE).

Auditory Steady State Response
The auditory steady-state response (ASSR) can be thought of as an electrophysiologic response to rapid auditory stimuli. The goal of ASSR is to create an estimated audiogram from which questions regarding hearing, hearing loss, and aural rehabilitation can be answered. Stimulus is modulated pure tone. Has potential to be a faster test than ABR when perfected. Some equipment can test multiple frequencies and both ears simultaneously. Uses same basic set-up and equipment as ABR.ASSR is similar to the Auditory Brainstem Response (ABR) in some respects. For example, ASSR and ABR record bioelectric activity from electrodes arranged in similar recording arrays. ASSR and ABR are both auditory evoked potentials. ASSR and ABR use acoustic stimuli delivered through insert earphones (preferably). ASSR is evoked using repeated sound stimuli presented at a high repetition rate, whereas ABR is evoked using brief sounds presented at a relatively low repetition rate.
